Milwaukee Journal Sentinel, by Mark Johnson, Kathleen Gallagher, Gary Porter, Lou Saldivar and Alison Sherwood

Lee C. Bollinger, President of Columbia University (left), presents the 2011 Explanatory Reporting prize to (l-r) Gary Porter, Kathleen Gallagher, Mark Johnson, Alison Sherwood and Lou Saldivar of the Milwaukee Journal Sentinel.
Winning Work
Desperate for clues to a 4-year-old's gut-destroying disease, doctors wonder whether a pioneering DNA technique could help.
By Mark Johnson and Kathleen Gallagher
Photos by Gary Porter
On a Saturday morning in June, when his children are at piano lessons and the Whitefish Bay house is quiet, pediatrician Alan Mayer composes the e-mail he hopes will persuade a colleague to try a costly new technology. He has been shaping the argument in his mind - the chance to take the first steps into the future of medicine and maybe save the life of a very sick little boy.
"Dear Howard - I hope you are well," he writes, addressing Howard Jacob, director of the Medical College of Wisconsin's Human and Molecular Genetics Center. "I'm writing to get your thoughts on a patient of mine . . . "
Nicholas Volker is a short, blue-eyed 4-year-old who loves Batman and squirt gun fights and steak - on the rare occasions when he's not restricted to a feeding tube.
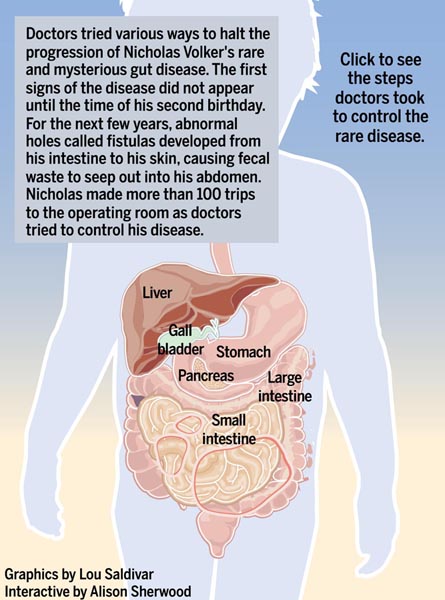
Food has become his dream - and his curse. Severely underweight, he arrived at Children's Hospital of Wisconsin in 2007 with the bony arms and distended belly of a famine victim. Yet when he ate, unusual holes would open between his intestine and skin, causing feces to leak into a large wound in his abdomen.
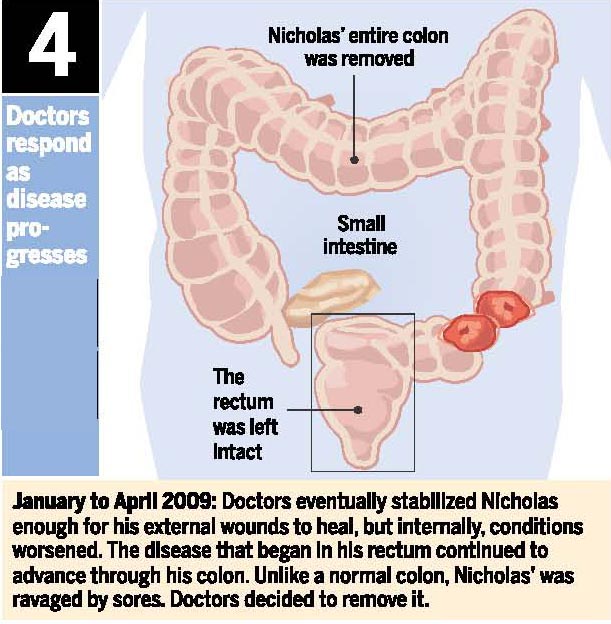
For two years he has suffered from this mysterious illness. He has survived more than 100 trips to the operating room. He has endured gut pains so severe he asked his mother to pray for him. Surgeons have removed his colon, its pink hue discolored by an enormous yellow ulcer.
The disease is relentless. Mayer and the other doctors have never seen anything like it. They have been unable to find another doctor anywhere who has observed the boy's affliction. Nor have they found the disease among millions of entries in the medical literature.
The case churns through Mayer's brain at night. He dreams of being lost in the woods and wakes with a tightness in his throat that comes from feeling responsible for another life.
A 44-year-old father of two with a background in genetics, Mayer has now arrived at what may be Nicholas' last hope.
"I am writing to ask if there is some way we can get his genome sequenced," he tells Jacob. "There is a good chance Nicholas has a genetic defect, and it is likely to be a new disease. Furthermore, a diagnosis soon could save his life and truly showcase personalized genomic medicine."
As he types that morning, June 27, 2009, Mayer realizes he is proposing a high-tech fishing expedition - the search for some mutation in a gene that explains the vicious disease he sees in the boy. They could spend months and tens of thousands of dollars only to find not one culprit, but a multitude among Nicholas' 21,000 or so genes. Even if they are lucky enough to find a single mutation, it is only a first step. They could discover the cause of the disease and learn they are helpless to treat it.
Mayer understands the uncertainties. They are outweighed by his responsibility to the boy and his faith that he'll know the right mutation when he sees it. The doctor rereads and polishes the e-mail until he is certain he has made his best case.
Then he hits "send."
***
Mayer's plea goes beyond one sick child. Reading Nicholas Volker's genes could change the way doctors treat patients, especially those whose symptoms don't match any known disease.
Even if the boy's illness affects just a handful of people around the world, the technique might be used to diagnose other rare, hereditary illnesses. Taken together, rare diseases, most of them hereditary, afflict 25 million to 30 million Americans, roughly one in 10.
The sequencing question also goes beyond standard medical research with its anonymous participants and far-off benefits. This time scientists would be trying to help a single child with a name and a desperate need.
Seldom has there been such urgency connected to the sequencing of one person's DNA. To this point, the technology has been used for research, or as a crystal ball to tell us whether we have a mutation that will lead later to a devastating disease such as Huntington's.
What Mayer needs is not a forecast, but an explanation for the disease Nicholas has today. Without it, he can only respond to symptoms.
The doctor has come to view the unknown illness as a dragon. All his skill has only lulled it into a temporary sleep.
"You want this dragon gone," he says.
***
From his office window at the Medical College, Howard Jacob can see Flight for Life helicopters land on the roof of nearby Froedtert Hospital. Urgency is something he understands.
For almost two decades Jacob has pushed to take our genetic code from the laboratory to the health care system. He imagines a day when doctors will read our DNA, review health risks, and devise ways of countering the defects and vulnerabilities each one of us has inherited.
But this is only a vision on the morning he reads Mayer's e-mail. His target for sequencing patients at the hospital is 2014, still an ambitious timetable. As of June 2009, there have been no published reports of patients diagnosed using this technology.
If sequencing enters the clinic in 2014, a new era in medicine will begin 61 years after James Watson and Francis Crick discovered DNA's structure, the spiraling strands, or double helix, that Crick called "the secret of life."
The new era would dawn some 40 years after Americans Walter Gilbert and Allan Maxam and Englishman Fred Sanger discovered different methods of reading the information on the double helix. They translated our genetic makeup into chains of chemical bases, a language of sentences and paragraphs written in a four-letter code: A for the base adenine; G for guanine; T for thymine and C for cytosine.
The new era would begin a little more than a decade after the Human Genome Project took the Gilbert-Maxam-Sanger discoveries to their logical extension by stringing together those sentences and paragraphs to produce the finished book, the first complete blueprint of a human being.
Jacob had played a major role in the 2004 sequencing of the first rat genome, significant because the vast majority of medicines are developed and tested using rats. He has seen the field move rapidly, especially in the last few years.
At presentations, he shows a slide of the machines that sequenced the first human genome. It took hundreds of machines seven years to accomplish the feat at a cost of $600 million. Today, a single machine at the Medical College accomplishes the job of 200 of the original human genome workhorses.
Sequencing a genome now takes a few months and costs tens of thousands, or hundreds of thousands of dollars, depending on the level of analysis.
Mayer's e-mail challenges Jacob and the Medical College to go beyond what can be done in theory or in several years.
If Nicholas Volker's disease continues, if doctors cannot discover the cause, he may not live to see 2014 and the grand plans Jacob has envisioned.
At the end of the e-mail is a link to the online journal kept by Amylynne Santiago Volker, Nicholas' mother. Read it, Mayer says, "and you will get a good flavor for the desperation of this situation."
Jacob has two children of his own. He clicks on the journal and reads.
***

Although Nicholas Volker has spent hundreds of days in the hospital, when he's well enough he goes to school in Monona. Nicholas holds the talking turtle as he tells his kindergarten class in April about his Make-A-Wish Foundation trip to Las Vegas over spring break.
The story begins October 26, 2004. The birth of a boy with a name as unique as his genes: Nicholas Zane Fernando Santiago Volker.
Amylynne, a homeschooling mom, and her husband, Sean, an electrician, choose "Nicholas" after the patron saint of children. The parents are Christians, regulars at their church in Madison. A silver cross dangles from Amylynne's neck.
Sean, a quiet, pickup truck and blue jeans kind of guy, has wanted a boy so badly - they have three girls - that before the birth, he would not allow Amylynne to pick female names. He sees himself tossing a football to his son, a Wisconsin boy through and through.
For almost two years, Nicholas appears healthy, the only sign of trouble, a certain pickiness about food. While he consumes breast milk, other foods repulse him. He lags on the growth charts.
Just before Nicholas' second birthday Amylynne discovers an abscess at the opening of his rectum. Doctors at the University of Wisconsin Children's Hospital in Madison give him antibiotics and the abscess bursts.
In its place, two holes appear. It does not seem to Amylynne that the doctors are worried initially, but she is sure something is wrong. She has grown up with doctors: her father, stepmother, two brothers and their wives, a sister and her husband.
Her fears are borne out. The two holes merge into a larger opening, and stool leaks through it.
But tests only tell the doctors what Nicholas does not have.
Eight months of visits to UW Children's Hospital bring a succession of medications.
No diagnosis.
***
The disease is relentless.
In early 2007, Amylynne takes Nicholas to a gastroenterologist at Children's Hospital of Wisconsin near Milwaukee for a second opinion. Subra Kugathasan has seen hundreds of patients with inflammatory bowel disease, but none like Nicholas.
The boy is much younger than most patients with such an illness. His symptoms resemble Crohn's disease, a type of inflammatory bowel disease. But Crohn's can be treated. Nicholas' disease cannot.
"He basically failed every single medical, surgical and nutritional approach," Kugathasan would say.
Amylynne likes Kugathasan for his gentleness. She forms a particular bond with Marjorie Arca, the pediatric surgeon who examines Nicholas' large intestine.
Arca fell in love with pediatrics years ago, the evening a sick 4-year-old gave her a Christmas ornament he'd made. Amylynne trusts her. Both women are Filipino. Both wear crosses. Most of all, Arca is thorough.
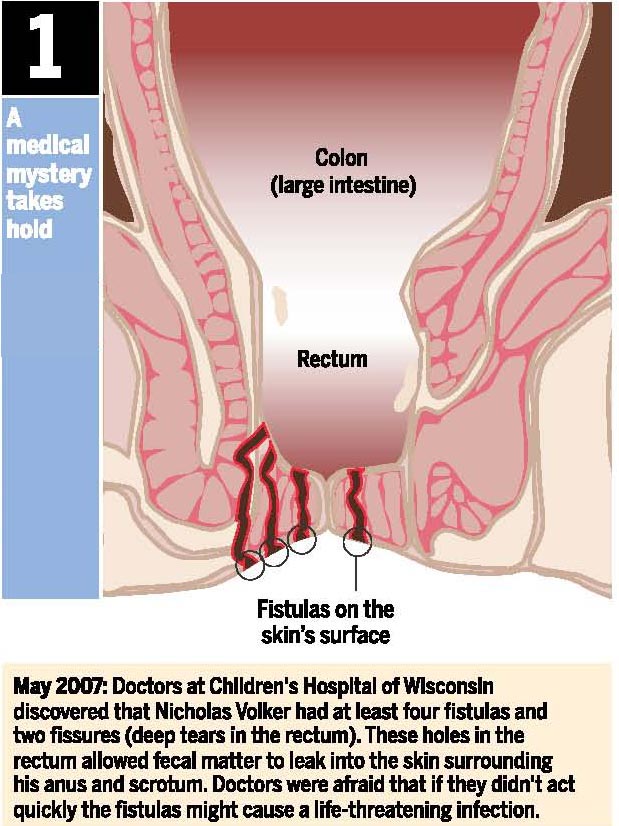
In her initial examination, the surgeon discovers that Nicholas now has four holes, pencil pricks drilled through the skin all the way into his intestine. That's why stool is leaking. Arca says the holes are called fistulas. Weeks earlier another doctor had found no fistulas.
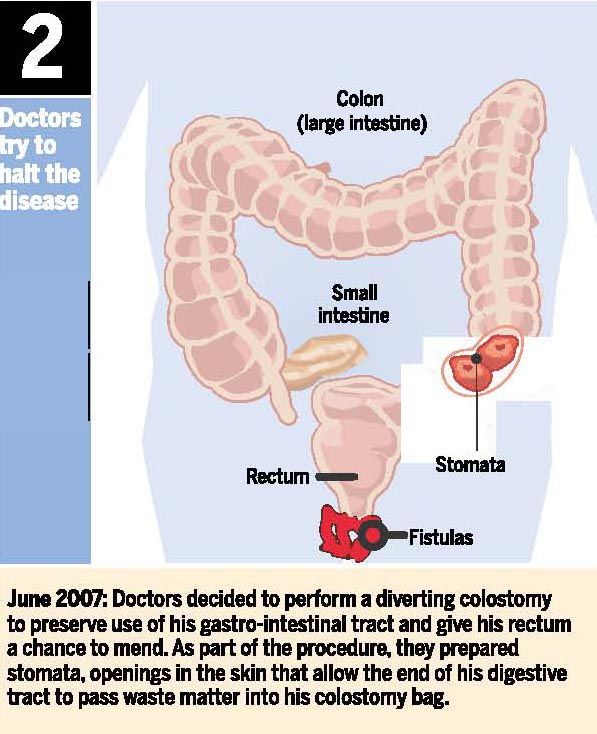
Arca performs a colostomy, diverting waste from his damaged intestine to a bag outside his stomach
Less than a month after the surgery, Nicholas has more fistulas. The skin surrounding the holes grows purple. By late June, Nicholas seems to be fading fast.
Doctors give him blood transfusions and a medication that spurs the production of infection-fighting white blood cells. Gradually his energy returns. He is playing with his trains again. His cheeks grow chubby. The fistulas heal.
On Sept. 1, 2007, he tells his mom he's not sick anymore.
***
Two days later, the Volkers race along I-94 from Madison, bound for the emergency room at Children's Hospital. In the back seat, Nicholas is hallucinating. He sees spiders on the ceiling.
He had been doing so well. Home from the hospital for the weekend. Blood counts good.
But Sunday his breathing had turned rapid and shallow. He had no energy. Amylynne felt his forehead; he was burning up.
She knew what was wrong. Nicholas had classic symptoms of sepsis, an often deadly blood infection.
As Sean drives, Amylynne sits in back comforting Nicholas. The boy is sweating, his pulse galloping. He mumbles and Amylynne prays aloud, the words flowing almost mechanically because there have been so many emergencies.
Oh Heavenly Father, I ask that you please protect Nic.
Children's Hospital confirms her fear. Nicholas has sepsis. For several weeks, her journal fills with worry. Sometimes others write the entries. While Sean works and cares for the girls, Amylynne seldom leaves her son's bedside. Although she is not supposed to, some nights she curls up beside him.
Nurses marvel at the way she pulls herself together each morning, applying makeup, dressing in business suits. She does not give up on anything, not even her appearance. No matter how grave the news.
Sept. 4.
"Nicky is in dire straits . . . He is at risk for all organs being damaged or failing now. His temp is now at 106 . . . "
Sept. 6.
"The doctors are asking her to make decisions about whether or not to resuscitate him if he would go into cardiac arrest . . . "
Sept. 13.
"Nicholas had a couple of breathing scares because of his collapsed lung . . . "
Sept. 20.
"Nicky is in day 5 of a very high fever which has reached as high as 105.6. He has tested positive for E. coli which has come from his breathing tube."
At times the situation is so serious that relatives talk to Amylynne about visiting a funeral home; she refuses. Her father encourages her to give a "do not resuscitate" order. Absolutely not, she says. I will not give up hope.
There is a word she won't write in her journal. She calls it "the D word."
In the end, there is no need for the word. After receiving powerful antibiotics and numerous transfusions of blood, plasma and platelets, the boy Amylynne calls her "little warrior" pulls through. A month after the crisis began, he is well enough to eat scrambled eggs, the first food in all that time that has not come through a tube. In late October, seven weeks after the sprint to the emergency room, Nicholas goes home.
Early in 2008, the inflammation and fistulas return.
***
The longer Nicholas' illness defies diagnosis, the more specialists weigh in. Half a dozen doctors now form the core of the boy's expanding medical team. They take home questions and hunches about him. At night, they search the medical literature. At conferences across the country, they tell colleagues about Patient X, the anonymous child with the mysterious disease.
"I thought he was going to be one of those kids who dies without us knowing the answer," Kugathasan would say.
Doctors run tests on individual genes and more tests on the immune system. One theory holds that Nicholas' immune system has turned against his body, killing healthy cells. Bill Grossman, an immunologist at Children's and the Medical College, spends hour after hour dissecting complex genetic pathways, hoping to understand what is happening inside the child's body.
"We did pretty much any test you can think of on him," Grossman says. "The more we got back, the more confusing the picture was. . . . He really was a one in a billion kind of case."
In August 2008, the Volkers seek another opinion, this time at Cincinnati Children's Hospital Medical Center, which has expertise in illnesses that resemble Nicholas'.
"He's certainly one of the sickest children we've seen," says Ted Denson, who is medical director of the hospital's center specializing in inflammatory bowel disease. "You needed to give him about twice as much nutrition as you'd normally give a child to get any weight gain at all."
The doctors in Cincinnati conduct numerous blood and genetic tests. They find no specific genetic cause. The best they can tell, Nicholas has an immune disorder. For some reason, white blood cells called lymphocytes have kicked into overdrive, destroying cells that line the intestinal wall. The Cincinnati hospital concludes that Nicholas must receive more nutrition until he is well enough to have his diseased colon removed.
By January 2009, Nicholas is back at Children's Hospital of Wisconsin. He is now 4 years old. He has been poked, prodded and jabbed with needles so often that sometimes he growls at the doctors and nurses.
He weighs less than 20 pounds, well below the 35 pounds of a typical 4-year-old.
No diagnosis.
***
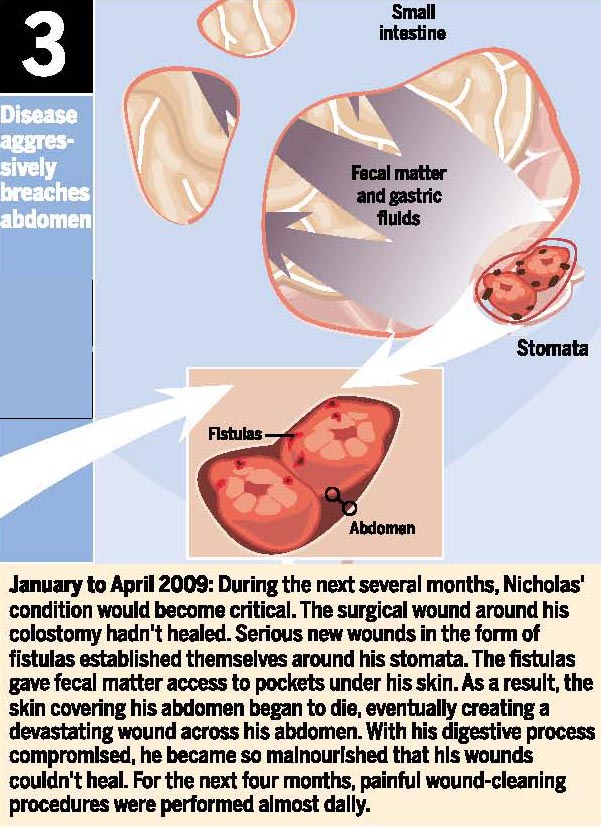
The gaping wound in Nicholas' abdomen from his colostomy will not heal. As the disease spreads from his bottom to his colon and small intestine, more holes form and stool drains through them into the wound, raising the threat of infection.
No article in a medical journal prepares a surgeon for such a wound. It must be cleaned and dressed so frequently that for several months Arca has a standing daily appointment with Nicholas in the operating room.
Although cleaning and dressing wounds is not usually considered surgery, in Nicholas' case the task takes at least two hours and requires general anesthesia.
They have a routine. Nicholas' mother carries him to the operating room, which she cannot enter without wearing scrubs. Arca meets her and carries the boy inside.
Often Nicholas wears his black Batman cape and mask. On his hands: Batman gloves that make the sound "Ka-pow!" He prefers to be called "Batman."
What should we listen to? Arca usually asks. Jonas Brothers?
Nicholas likes the Jonas Brothers. His mother has heard him sing: "A little bit longer and I'll be fine."
He holds out the tube in his chest, used for medications, fluids and blood draws.
I would like milky Versed, he says. That's what he calls the anesthetic propofol (it reminds him of Versed, a sedation drug).
He chooses a flavor for the oxygen he receives. Today it's blueberry.
I'll hold the mask, he says. If residents try, he pushes them away.
When it is over and his eyes open in the recovery area, Nicholas always asks for Mom.
***
By summer 2009, Nicholas has spent more than 300 days at Children's Hospital. Time enough for Kugathasan to move to a hospital in Atlanta and Grossman to move to a pharmaceutical company. Time enough for Kugathasan to be replaced by Michael Stephens, a gastroenterologist, who is replaced by Mayer.
Time enough for one of the nurses, Tara Bell, to find she is caring for Nicholas not only at work but in her dreams.
The wound in his abdomen heals after his inflamed colon is removed. Still, the boy's health rises and falls so often and the lack of a diagnosis persists so long that conflicts between the Volkers and their medical team become inevitable. Getting Nicholas to gain weight without sprouting new fistulas becomes a personal mission for Mayer. At times when they disagree, Amylynne reminds him: "He's not your child. He's my child."
She has learned to care for Nicholas outside the hospital. Years ago, she had been squeamish to the point of throwing up at the sight of excrement and had declined her father's wish that she attend nursing school. Now she changes colostomy bags and flushes and maintains intravenous lines. She considers becoming a nurse.
Nicholas' three sisters, all teenagers, think of their brother at school when friends mention younger siblings. They miss the crazy things he says, and even the way he gets them to compete for the honor of favorite sister.
Sean endures long absences from his son for the first two years of the illness, taking all the overtime he can get to pay what health insurance will not. Then, in the early months of 2009, the construction jobs dry up and he and Amylynne swap roles. He goes to the hospital; she does clerical work for Great Wolf Resorts.
The father and son grow close, passing long hours in the hospital room playing on the floor and talking superheroes and monster trucks. When Sean returns to construction sites, he thinks back to those days, and sometimes his phone rings and it is Nicholas' high-pitched voice: Dad, when are you coming?
The long hospital stays get to Nicholas most of all. Amylynne sees the way he grows so familiar with the different floors that the hospital becomes a de facto home, the way he longs for friends and enjoys "hospital play dates," the way his friends always leave. They go home after a few weeks, or they die.
Months have passed since the last time Nicholas ate real food. He tells a nurse about the steak he will eat when he goes home. At night, he sleeps with a bag of Bagel Bites cradled in his arms.
There are days Nicholas asks:
Mom, is God listening?
Is He there?
Because, why would I be here then?
Sometimes Amylynne tells him: God is always with us. Sometimes the questions leave her speechless, wiping away tears.
By now she is desperate to cure Nicholas herself. After doctors suggest he may need a bone marrow transplant, Amylynne talks with Sean about having a baby to serve as the donor (no one in their blended family is a genetic match for Nicholas). Her pastor dissuades her, saying that she would be forcing a solution rather than trusting God to provide one.
So when Mayer suggests sequencing Nicholas' DNA, she is ready.
The cost will be high. Even if insurance did pay for such things, Nicholas has exceeded his $2 million lifetime benefit. Money will have to be raised.
Reading his DNA will have implications for the family. Nicholas' genetic information comes from his parents; examining it will reveal things about them and about their relatives. Doctors seeking the cause of Nicholas' gut disease could find mutations for other illnesses that run in families.
None of that worries Amylynne. What matters is Nicholas.
***
The mother's journal is 230 pages and growing. A book with no end in sight.
As he reads, Howard Jacob, head of the Medical College's genetics center, wonders what it would be like to watch one of his children wheeled into the operating room.
He imagines his child disappearing behind a door where he can neither follow nor offer protection. Then he tries to imagine experiencing that moment more than 100 times, as the Volkers have.
Jacob knows the chances of finding the cause of Nicholas' illness - perhaps one mutation hidden among thousands of minor variations in his genetic script - are slim to none. He knows, too, that without a diagnosis the boy's long-term odds are little better.
He must weigh the two. The risk that an ambitious test of a new technology could fail. The risk that if they do not make the attempt, a young boy could die.
Jacob recalls what he tells his students. You do the experiment because you need to do it.
There is no other way to learn whether something works.
Coming Wednesday: Researchers seek clues in Nicholas' DNA - and find more than they expected.
Glossary
By Mark Johnson
Abscess: An area in which pus has accumulated in a newly formed cavity.
Adenine: One of four bases that are chemical components of DNA.
Adenovirus: A virus that most commonly causes respiratory illness. Adenovirus may also cause other illnesses, such as gastroenteritis, conjunctivitis and cystitis (bladder infection).
Allele: One of the alternative forms of a gene. These forms differ in their sequence of DNA. There are usually two alleles of any one gene; one from the mother, the other from the father. One allele is often dominant, the other recessive. The dominant allele determines the characteristic that appears - for example, brown hair instead of blond.
Amino acid: Chains of these organic compounds form proteins.
Autoimmune disease: A disease in which the immune system becomes overly active, attacking the body's own cells.
Bone marrow transplant: A procedure that delivers healthy blood-producing stem cells into the patient. The cells replace bone marrow that is either not working properly or has been destroyed by chemotherapy or radiation. Some transplants use a patient's own cells to, in effect, reboot the immune system. Other transplants use cells from a donor to build a brand-new immune system.
Chromosome: A threadlike structure found inside the nucleus of a cell. It carries the genes. In humans, each cell contains 46 chromosomes.
CMV: Cytomegalovirus is a common virus that infects most people during their lives but rarely causes illness. Most people don't have symptoms, but the virus can resemble infectious mononucleosis accompanied by fever, swollen glands and fatigue. People with a compromised immune system may experience more serious illness involving fever, pneumonia and other symptoms.
Colostomy: A surgical procedure that creates an alternate channel for feces to leave the body. The surgeon brings one end of the large intestine out through the abdominal wall. As a result, stool moves through the intestine and drains into a bag outside the abdomen.
Crohn's disease: A disease that causes inflammation of the digestive tract and can produce diarrhea, vomiting, abdominal pain and weight loss. The disease can affect any part of the gastrointestinal tract from the mouth to the anus but usually affects the lower intestine. The cause of the disease is unknown, but one popular theory holds that the immune system attacks the gastrointestinal tract.
Cytosine: One of four bases that are chemical components of DNA.
DNA: This stands for deoxyribonucleic acid, the genetic material of most living organisms. It is a major part of the chromosomes inside the nucleus of a cell and determines hereditary characteristics.
DNA microarray: Technology used to measure changes in expression levels of genes and to detect variations in the genetic script called single nucleotide polymorphisms, or SNPs, as well as to genotype or resequence mutant genomes.
DNA sequencing: Method used to determine the precise order of chemical bases - adenine, guanine, cytosine and thymine - in a molecule of DNA. The order of those bases determines a person's unique assortment of genetic traits, risks and predispositions.
Double helix: The paired strands of DNA. The two strands run in opposite directions. The bases at each point complement each other. Adenine on one strand always matches thymine at the same position on the other strand. Guanine on one strand matches cytosine at the same position on the other.
Encephalitis: An acute inflammation of the brain
Exome: The part of the genome composed of all the exons.
Exon: The part of a gene that carries instructions for making a protein.
Fistula: An abnormal hole or passage in tissue.
Gain-of-function mutation: A mutation that causes a protein to take on a new or enhanced function.
Genetics: The scientific study of heredity and variation.
Genetic carrier: A person or organism that has inherited a genetic trait or mutation but does not have symptoms of the disease or traits caused by the mutation. Carriers can pass those traits or mutations to their offspring.
Genetic pathway: A set of genes that interact and work together.
Genome: All of an organism's hereditary information. To sequence the genome, scientists must determine the precise order of about 3.2 billion pairs of bases on the DNA double helix.
Genomics: The study not just of single genes, but rather of the functions and interactions of all genes.
Genotype: The genetic composition of an organism. A person's complete collection of genes. Also a verb, referring to the process of putting together a person's genotype.
Graft-versus-host disease: A common complication of bone marrow transplants. The transplanted cells regard the transplant recipient's cells as "foreign" and attack them.
Guanine: One of four bases that are chemical components of DNA.
Haploinsufficiency: This occurs when an organism only has a single functional copy of a gene and one functioning copy does not produce enough of the gene product (i.e., a protein), leading to an abnormal or diseased state.
Haplotype: A combination of alleles, or alternative DNA sequences, at multiple locations that are transmitted together on the same chromosome. These are inherited by an individual from one of its parents.
Hemizygous: Describes an individual who has only a single copy of a gene instead of the customary two copies. All of the genes on the single X chromosome in males are in the hemizygous state.
Heterozygous: Describes an individual who has two different alleles for a single trait.
Homozygous: Describes an individual who has received two identical copies of the same allele for a single trait.
HHV-6: Human herpesvirus 6 is a virus that can cause encephalitis and seizures.
Inflammatory bowel disease: A group of disorders in which the intestines become inflamed (red and swollen). Ulcerative colitis and Crohn's disease are examples.
Loss-of-function mutation: A mutation that reduces the production and/or function of a protein.
Lymphocyte: A white blood cell that functions as part of the immune system.
Mutation: A random change in the genetic material of a cell that may cause it to look or behave differently. Geneticists generally use the term when a change is both rare and harmful.
Nucleotide: Any of a group of molecules that when linked together form the building blocks of DNA and RNA.
Phenotype: The observable characteristics of an organism, based on genetic and environmental influences.
Proband: A person or animal being studied or reported on in genetic research. Sometimes refers to the first affected member of a family seeking medical help for some kind of genetic disorder.
RNA: Ribonucleic acid is an essential component of all cells. Its structure and sequence of chemical bases determine the important process of manufacturing proteins and also transmit genetic information.
Sepsis: An infection of the blood or soft tissue.
SNP: Single-nucleotide polymorphism, a DNA sequence variation that occurs when one nucleotide - adenine, thymine, cytosine or guanine - in the genome differs between members of the same species, or even between paired chromosomes in an individual. The variation can affect disease development.
Staph infection: An infection caused by staphylococcus, a group of bacteria. Staphylococcus can infect various tissues of the body. Staph-related illnesses can range from mild, requiring no treatment, to severe and potentially fatal.
Thymine: One of four bases that are chemical components of DNA.
Umbilical cord blood transplant: A transplant of blood that remains in the placenta or umbilical cord after childbirth. The blood is rich in stem cells that build the immune system. Cord blood transplants are considered an alternative to bone marrow transplants. Some doctors prefer umbilical cord blood because they believe it carries less risk of graft-versus-host disease.
Variation: A difference in the genetic sequence that can be good, bad or neutral.
X chromosome: One of the two sex-determining chromosomes. The other is the Y chromosome. Females have two Xs; males have an X and Y.
XIAP: X-linked inhibitor of apoptosis protein, a gene found on the X chromosome that provides instructions for making a protein found in many types of cells, including immune cells. It helps protect these cells from self-destructing by blocking the action of certain enzymes.
XLP: X-linked lymphoproliferative disorder is an inherited immune system disorder that affects fewer than 1 in a million children. The disorder is found on the X chromosome, only strikes boys and is usually fatal, rendering them unable to survive one of the most common human viruses, Epstein-Barr.
Sources: "A Dictionary of Biology," Oxford University Press; "Oxford Dictionary of Science"; "DNA: The Secret of Life," by James Watson; Wikipedia
About this series
This series began with a tip in January, two months before the case became public. Medical College of Wisconsin experts had sequenced the DNA of a young boy at Children's Hospital of Wisconsin. In early 2010 only one other case of doctors sequencing a patient's genes to obtain a diagnosis had been reported in medical literature, and it had received little attention in the popular press.
Reporters Mark Johnson and Kathleen Gallagher received permission from Nicholas Volker's family, the hospital and the Medical College to tell the story of how Nicholas' genes were sequenced and how doctors used the information to treat him. The reporters interviewed more than 60 people, including members of the Volker family, the doctors and nurses who treated Nicholas, the scientists who handled, sequenced and analyzed his DNA sample, and experts in genomic medicine.
They also accompanied Nicholas to doctor appointments. Reporters visited a lab at the Medical College to watch scientists sequence DNA.
A number of written sources were used. The reporters read Amylynne Volker's 500-page online journal chronicling more than three years of her son's treatment. In addition, they read James Watson's "DNA: The Secret of Life," and more than three dozen medical and scientific papers.
Some scenes described in the series were witnessed by the reporters. Other scenes that took place before 2010 were reconstructed based on extensive interviews with the participants and accounts in Amylynne Volker's journal.
© Milwaukee Journal Sentinal
By Lou Saldivar and Alison Sherwood
Can scientists pinpoint Nicholas' devastating gene mutation -- and quickly?
By Mark Johnson and Kathleen Gallagher
Photos by Gary Porter
James Verbsky is drawn to pediatrics by its ethical simplicity - the notion that you do anything to save a child. Yet as the doctor talks with colleagues at Children's Hospital of Wisconsin in the summer of 2009, he finds himself doubting their proposal for 4-year-old Nicholas Volker. They want to sequence Nicholas' DNA.
The boy in the Batman cape has a mysterious disease marked by painful holes leading from his intestine to his skin. Fecal matter leaks through the holes. In 2 1/2 years, Nicholas has made more than 100 trips to the operating room.
Verbsky, a 39-year-old immune specialist, has run every test he can think of to pin down the source of Nicholas' disease. So have the other doctors. They are running out of options.
Some favor a bone marrow transplant based on the theory that Nicholas' immune system has gone out of control and is destroying healthy cells. But the procedure is risky and the doctors are not certain it will help. How can they be certain? They don't understand the problem they're trying to fix.
Verbsky's colleagues hope the answer can be found by reading the boy's genetic script. But the hospital and the Medical College of Wisconsin have never sequenced all of a patient's genes and were not planning to until 2014.
To do so for Nicholas could take months, cost a small fortune and still leave more questions than answers.
Every human carries thousands of variations in the genetic script, the long chain of chemical bases that makes us who we are. These differences - the base adenine in one position instead of guanine - determine everything from harmless diversity (brown hair vs. blond) to the defects that cause disease. Although some differences are harmful, most are not. Some are even beneficial.
They could find 20,000 of these differences in Nicholas' genome, Verbsky worries, so many that they will never determine which of them caused his illness.
"I was skeptical when they said they were going to sequence him," he would later say. "I laughed, to be totally honest."
***
Soon after the July Fourth weekend, 10 doctors and scientists meet at the Medical College to discuss sequencing Nicholas. The man who called the meeting, Howard Jacob, head of the Human and Molecular Genetics Center, has never met Nicholas. He has been weighing whether to sequence him for a little more than a week, ever since the boy's pediatrician, Alan Mayer, suggested the idea.
Although Jacob can find no published reports of a patient being sequenced to diagnose a disease, when he reads the spirit in the room he finds a willingness to try.
Mike Tschannen (pronounced Shannon), the research associate who runs the college's sequencing lab, looks at the question this way: "If we choose not to do this, why are we here? This is the entire reason we're here."
The scientists decide not to read Nicholas' entire genome, a massive undertaking that could cost up to $2 million. Instead, they plan to target a little more than 1%, the exons. Part of every gene, exons carry the instructions for making proteins. It is the failure to make proteins correctly that causes many diseases.
While zooming in on this section of the genome cuts the cost substantially, the estimate is not trivial: $75,000. Donors will have to be found.
The Medical College, a relatively small player in genomics with just one sequencing machine, will be attempting something that large centers with dozens of machines have not done.
As they leave the conference room that day, one of the most optimistic is Liz Worthey, a senior research scientist from Scotland. Since the moment she learned of the project, she has felt: We can do it. Now, she will be called upon to make sense of the thousands of variations they expect to find in Nicholas' genetic sequence.
The project will be different from anything Worthey has ever done. As a researcher, she is accustomed to thinking that her work may affect thousands of people, years in the future. This time she may help a single child.
This time she does not have the luxury of years.
***
"We need urgent prayers now please," Nicholas' mother, Amylynne Santiago Volker, writes in her online journal.
It is July 14, 2009. She has received worrisome news.
Two of the doctors, David Margolis, a bone marrow transplant specialist, and James Casper, a blood expert, are recommending giving Nicholas very high doses of chemotherapy, a treatment that has proved successful in children with Crohn's disease. Unable to reach a definitive explanation for Nicholas' illness, the doctors have settled on Crohn's as a working diagnosis.
If he survives the chemotherapy - and the doctors believe he will - the hope is that the drugs will wipe out his immune system, allowing it to reset and develop normally this time.
Amylynne cannot get past the "if." Too many times in the last few years, she has been warned that Nicholas might not live out the night.
She leans heavily on her faith. Yet she cannot ward off the fear that something will go wrong.
At this point, DNA sequencing is not her focus. Doctors are asking that she decide on the chemotherapy plan soon, before Nicholas becomes too sick for treatment.
"What do I choose?" she writes. "How do I make the right decision? What if I wait? What if I don't wait? Either way I could compromise my son's life."
***
The sequencing of Nicholas' DNA begins with money and paperwork and blood.
In addition to its scientific challenges, the project straddles a sensitive regulatory border. Is it research for the greater good, or treatment for a single patient?
Children's Hospital has a rule prohibiting staff from raising money to pay for the care of one patient. But Howard Jacob says that's not what he's doing. He is raising money to run a pilot test of sequencing because the technology has the potential to help many patients.
The interpretation differs when pediatrician Mayer consults the hospital's institutional review board. The board oversees human subject research, but this is not research, says chairman Paul Scott. Reading Nicholas' DNA is an attempt to help one patient; it is nothing more than the practice of medicine.
In fact, sequencing is both: a way to help Nicholas, and to test a technology that could help others. But before the project can proceed, money must be raised, a task for which Jacob is well-positioned. He speaks to business groups frequently and co-founded a start-up company, PhysioGenix, which helps drug developers test their compounds.
Once Jacob begins making calls, it does not take him long to raise the money. In addition, the company that makes the sequencing machine decides to collaborate with the Medical College team by performing the first run for free.
Amylynne Volker is hopeful, though she has been warned that sequencing may not reveal an answer. Nicholas has undergone many tests already: at least nine focusing on individual genes and 35 examining his immune system. And still, no diagnosis.
Before sequencing can begin, Amylynne must sign a stack of releases, so many pages she does not read most of them. Then medical staff go to her son for blood, a more efficient source of DNA than saliva. All they need is a teaspoon.
***
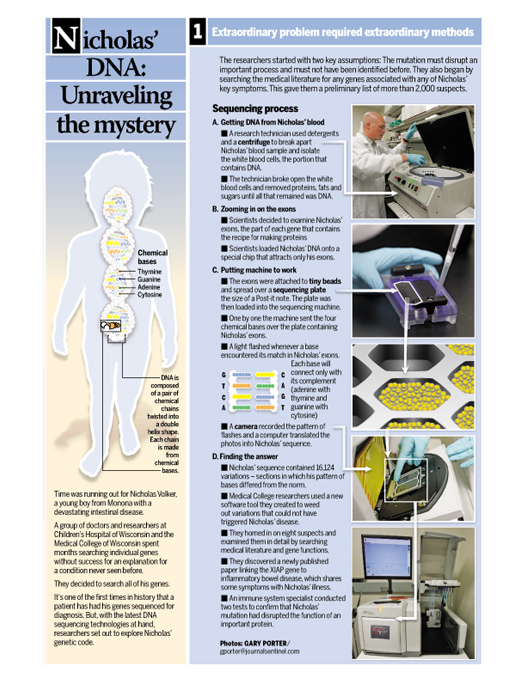
If the disease is genetic, the clues lie packed inside the nuclei of Nicholas' white blood cells, the portion of his blood sample that contains DNA. First, scientists must remove the red blood cells, platelets and plasma.
Although there is a machine that can extract DNA, the individual strands emerge in better shape when the job is done by hand. Mike Tschannen, who runs the sequencing lab, knows the hands he wants working with Nicholas' blood. He goes to Gwen Shadley, a research technologist at the Medical College who has a talent for pulling good DNA from samples.
Tschannen does not tell her whom the blood comes from, whether the person is alive or dead. Only this: Handle it with tender loving care. It's a very special sample.
Shadley first uses a solution to burst the red blood cells, then a centrifuge to separate out the plasma, platelets and cell debris. At the bottom of the test tube are the white blood cells. She adds detergents to break open those cells, releasing the DNA inside. Then she separates out the other cell contents - proteins, sugars, fats. What's left gets poured into a test tube of alcohol solution. She places the tube on a machine that rocks gently back and forth.
Tiny strands of DNA like fine white thread drift through the solution and clump together, all visible to the naked eye.
"It's absolutely gorgeous to see," Shadley says. "I was born and raised on a farm. It's almost like watching a birth."
Within 24 hours Nicholas' blood is pared down to DNA, his genetic secrets reduced to a clear, ordinary-looking liquid.
Tschannen places a large drop of the liquid inside a sealed container surrounded by dry ice and sends it by overnight mail to the pharmaceutical giant Roche.
The company's 454 Life Sciences division is performing the first sequencing run. Technicians begin by breaking the long strands of DNA with their 3.2 billion chemical base pairs into shorter, readable stretches. Using pressurized nitrogen gas, they shear Nicholas' DNA into segments of roughly 500 to 800 bases.
The segments are loaded onto a special chip the size of a microscope slide that captures only the exons. Whatever does not stick to the chip - the non-exon portion - is washed away
Nicholas' exons are attached to tiny beads and spread over a sequencing plate the size of a standard Post-it note. The plate is then loaded into the machine.
The sequencing machine works by reading individual segments, then reassembling them into the complete string.
One by one each of the four bases - adenine, thymine, guanine, cytosine, or A, T, G, C - washes over the plate containing Nicholas' exons. A light flashes each time the base encounters a match. A matches T; G matches C.
A camera photographs the pattern of light flashes.
A computer translates the photos into Nicholas' sequence.
***
Meanwhile, Worthey and research scientist Stan Laulederkind get an early sense of the best candidates to cause an illness like Nicholas'. They scan the medical literature for papers that tie specific genes to any of the boy's symptoms. Whenever a pathway - a group of interacting genes - is linked to a symptom, they include all of the genes.
By August, a month or so into the sequencing project, their finished list contains more than 2,000 suspects. Doctors are confident one is the gene they're hunting. Yet they know the machine will produce a much longer list of possibilities.
To prepare for the deluge, Worthey and David Dimmock, a pediatric genetics specialist at Children's and the Medical College, devise a strategy to narrow down the thousands of differences they expect to find between Nicholas' sequence and what is considered normal. To this point relatively few human genomes have been read, so "normal" has yet to be fully established.
The Medical College team is guided by two assumptions: The crucial difference in Nicholas' DNA, the one at the root of his disease, must sabotage an important process in the body and must have been undiscovered until now, since Nicholas' disease does not appear in medical literature.
To find it they must eliminate the differences that do not have dire consequences. Some produce the same amino acid as the normal sequence. Others change an amino acid but do not disrupt a vital function in the body.
Existing tools can analyze some effects of these differences. But scientists have nothing that can perform the broad analysis Worthey and her colleagues require.
So she designs her own tool. Working with a group of software developers at the Medical College, she pulls together new and existing algorithms and data from different sources to create a program that can tackle a case of Nicholas' complexity. She calls the program Carpe Novo, Latin for "seize the new." Carpe Novo is still being developed in August when the results arrive from the first read of Nicholas' DNA.
James Verbsky's initial fear that they would find 20,000 variations was not far off. In all, Nicholas has 16,124.
That's the size of the haystack they're searching.
**
Late in August, Nicholas is receiving high doses of chemotherapy, the treatment doctors have recommended. The treatment Amylynne has been dreading. His fever hovers around 104. He vomits up to 20 times in a single day.
When Nicholas looks into a hand mirror he sees his head, bald from the chemo. He shrugs and walks away. He wants to go home.
Finally, in early September, his pediatrician calls with the first good news in months.
"NIC IS IN REMISSION," Amylynne writes in her journal. "PRAISE GOD!!!!"
After 250 consecutive days in the hospital, he returns home to Monona, a Madison suburb. He enjoys the simple pleasures of jumping in leaf piles, riding the bus to 4-year-old kindergarten, and trick-or-treating with Batgirl (his mom) and Wonder Woman and Robingirl (two of his sisters). He can even eat - as long as he adds just one new food a week, Mayer says.
One day that fall, Amylynne writes in her journal, "Now he is dancing in front of the television, eating some kind of sticky treat."
***
Somewhere in a pool of 16,000 variations in Nicholas' genetic script lurks the cause of his disease, if only Worthey and Dimmock can find it.
Dimmock, an Englishman, discovered his passion for pediatrics in the resiliency of the children he cared for a decade ago at a tin-roofed hospital in Uganda. He would treat them for malaria one day, and watch them race across the hospital grounds the next.
For more than a year, Worthey and Dimmock have worked together on research using sequencing to understand the genetics of liver failure and the genes that cause mitochondrial disease. But Dimmock has not lived solely in the research world with its slow progress toward conclusions. He screens babies for metabolic diseases and sees children born with genetic conditions. He knows what it means to need a diagnosis yesterday.
Although their roles blend at times, Worthey is the data-miner, Dimmock, the clinician. She gets computers to pry information from Nicholas' lengthy genetic script; he compares potential mutations with the boy's clinical profile.
Based on the results from the first sequencing run, they list variations in 32 genes that appear promising.
Two raise particular interest: a gene called CLECL1 and another called XIAP, both involved in regulating the immune system. CLECL1 was among the more interesting suspects on Worthey's list of 2,000-plus genes; XIAP did not make the list.
Not all genes are captured in one sequencing run, so they must repeat the process several times. Each run is like a slide superimposed over the previous slides, adding depth and resolution to the picture. After the first run at Roche, Nicholas' DNA passes through the sequencing machine at the Medical College four times.
To this point, Mike Tschannen has used the Medical College machine solely for research, sequencing rats and bacteria and examining a few specific areas of human biology. Now, he sees a chance to show that a small lab with one machine "can do science that may change the world."
In an eight-day span at the end of September, Tschannen works 92 hours sequencing Nicholas' DNA three times. In early October, he performs one final run.
Multiple copies of each short segment of DNA pass through the machine on each run. After five runs, each segment of Nicholas' DNA has been read an average of 34 times, enough to reduce significantly the possibility that a mutation could be missed.
Worthey and Dimmock filter Nicholas' variations with the software tool and search a database of genetic differences. They discover that many of his variations, including CLECL1, are common and can be eliminated.
Their list drops to eight.
Worthey examines what each gene does and conducts a more thorough literature search. She zeros in on two genes, then discovers that one, GSTM1, is commonly altered in people who are perfectly healthy.
That leaves one prime suspect: XIAP.
Since the previous literature search two months ago, a new article has appeared in the Proceedings of the National Academy of Sciences linking XIAP to a pathway involved in inflammatory bowel disease. Several of Nicholas' symptoms resemble that disease.
It is now November 2009. Worthey scans the publicly available human genome sequences. Then she goes further, asking researchers with unpublished genome data to look for this variation in XIAP. In all she is able to check about 2,000 human genomes.
Not a single one has the variation.
It must be Nicholas' mutation.
For the first time, his disease begins to make sense. If Worthey and Dimmock are correct, the holes in Nicholas' intestine, the ravaged colon, all of it stems from a single misplaced base in the long chain of his DNA.
On the X chromosome, on the gene XIAP, the rest of humanity has the sequence thymine-guanine-thymine.
Nicholas has thymine-adenine-thymine. In the single-letter shorthand scientists use, he has what amounts to a typo, an A instead of a G.
The bases in this sequence make an amino acid, the 203rd in a chain of almost 500. That amino acid is supposed to be cysteine, and has been in all humans examined to this point.
But in Nicholas, the one-letter change produces an entirely different amino acid, tyrosine.
His tyrosine is part of a long chain that makes a protein, also called XIAP. This protein has two important jobs: it blocks a process that makes cells die and it helps prevent the immune system from attacking our intestine.
In Nicholas, however, the protein is made incorrectly. In his body, the immune system is at war with his intestine.
Since the human genome is composed of more than 3 billion base pairs, Nicholas' mutation represents the smallest possible error in a vast blueprint. Imagine one letter out of place in the 55 million-word Encyclopaedia Britannica online edition.
Even this image does not do justice to Nicholas' terrible luck. Not only is his misspelling unique among the human genomes examined, it is unique among the animal genomes Worthey checks. Fruit flies, rats, mice, cows, chickens, chimpanzees - every organism she can find makes cysteine at this position.
To Worthey, the extreme rarity of his mutation across the species carries an unmistakable message.
"If all of those organisms have (cysteine) at that position, then clearly it's important because over all that time it has never been allowed to change," she says, "(If it did) something bad obviously happened to stop that line from evolving any further. So everything has a cysteine."
Except Nicholas.
***
On a Friday afternoon in mid-November, Amylynne's cell phone rings. It is Mayer, Nicholas' pediatrician.
Has anybody contacted you from the hospital? he asks.
Nicholas and Amylynne have been home for six weeks. Nicholas, now 5, has been going to school, playing, eating.
Mayer says the doctors are excited. They have found the mutation. Maybe.
From the beginning, Mayer has felt he would know the right mutation when he saw it. After reading the paper on XIAP, he is confident they have their culprit. Still, he is cautious with Amylynne.
Her mind skims over the new information.
All right, she says, what disease? How many years does Nic have to live? Tell me the bad news first.
Mayer explains that a mutation on Nicholas' X chromosome has caused the illness in his gut. But there's more. The same mutation has also caused a second extremely rare disease called XLP. Only boys get this second disease, which leaves them unable to fight off one of the most common human viruses, Epstein-Barr.
Most die before the age of 10. The only cure is a bone marrow transplant.
A few days later, Amylynne meets with Dimmock, the genetics specialist. He explains what the doctors have found, and why it leads them to believe Nicholas needs a bone marrow transplant, a risky procedure that had been under consideration before the sequencing. First, Nicholas' blood must be sent to a federally approved clinical lab to confirm the mutation.
Dimmock tells Amylynne that he would like to test her blood to determine whether she has the same mutation. Some mutations are not inherited but occur as the egg forms.
The doctor explains that what they find may have implications for her children and other relatives. They may learn what the likelihood is that they have the mutation and could pass it to their own children.
Dimmock goes through the consents that must be signed, and asks a series of questions.
Are you Nicholas' mother?
Really? Amylynne says. You're asking me if I'm the mom?
Is Sean Nicholas' father?
Yes and Yes.
Although the questions seem odd and uncomfortable, the need to ask them is not far-fetched. Doctors have learned that a proportion of tests for genetic diseases inadvertently disclose unsettling information, for example, that Dad isn't actually Dad. DNA tells our secrets.
Finally, Amylynne must answer two questions: Does she want her own DNA tested, and does she want to know the results?
Yes and Yes.
***
In early December 2009,the boy's disease reawakens.
Nicholas loses weight. He becomes lethargic. The Volkers worry about swine flu or mononucleosis. They take Nicholas to Children's, hoping he won't have to spend another Christmas there.
Amylynne has moved into a room at the Ronald McDonald House near the hospital. She buries her head in a pillow.
"This must be what hell is like," she writes in her journal.
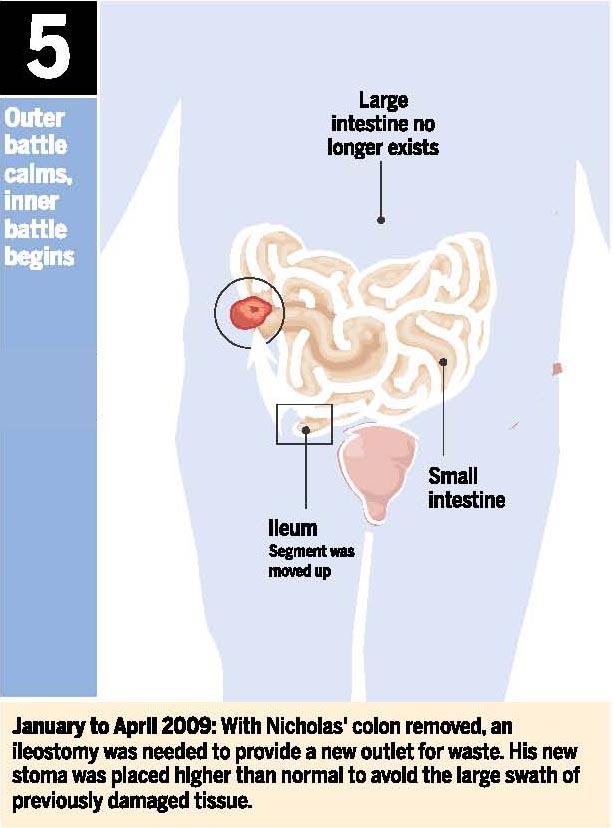
Nicholas' ileum, the final section of his small intestine, is full of pus and ulcers. Amylynne worries he'll never eat again.
A few days before Christmas, Nicholas erupts.
"I want my food back. Give me my food back," he screams, an outburst Amylynne records in her journal. "I don't want to get better, I want to be sick and have my food."
***
It falls to the skeptic to prove that sequencing has worked.
Despite his early reservations about the technique, James Verbsky feels a rush of excitement when he learns a mutation has been found and confirmed by the clinical lab. The fact that the mutation is unprecedented, that evolution appears to have kept it from taking hold in other species, tells him that in all likelihood they have found the culprit.
Still, the immune specialist knows the scientists need more evidence before they can say that this defect caused Nicholas' disease. They must show the mutation prevents the XIAP protein from doing its job.
To do this, Verbsky designs two tests. In one, they stimulate Nicholas' cells, adding a product made by bacteria to see whether the cells will recognize it and respond, as they should, by releasing a protein. Three times they perform the test. Each time other human cells release the protein.
Nicholas' cells do not.
In the second test, Verbsky and his team try to determine whether Nicholas' XIAP protein is curbing a process that causes cells to die. Once again Nicholas' cells differ from other human cells. More of his cells die. His protein isn't saving them as it should.
Now, Verbsky believes, they have the evidence. The single-letter mutation prevents Nicholas' protein from performing its jobs; that is why his gut doesn't work. The answer, so logical yet unexpected, prompts the scientist to reconsider the future of the test he once doubted.
To this point, doctors facing a mysterious condition would often single out suspicious genes and test them one by one. Each genetic test could take two to three months and cost up to $3,000.
Sequencing now gives medicine the chance to dispense with piecemeal methods and examine all of the genes at once. While it has cost roughly $75,000 to sequence and sift through Nicholas' DNA, the price is plummeting and should reach $1,000 or less in a few years.
"In five years," Verbsky says, "this is what we will do. I have no doubt."
***
Early in 2010, Amylynne returns for a second meeting with Dimmock. The tests on her DNA and immune system are complete.
The doctor begins with a preamble, one he always gives before genetic testing and again when the results come back. We have no say in the genes we pass to our children. There are benefits to reading our DNA, but they are balanced by the potential harm of what the DNA tells us.
Then the preamble is over.
You carry the mutation, he says.
Like all females, Amylynne has two X chromosomes. One has the normal gene; the other has the mutation. The normal X appears to compensate for the bad X. That's why she is not afflicted with her son's disease.
Like all males, Nicholas has only one X chromosome. It has the mutation.
Amylynne's eyes fill with tears.
The doctor is saying she did not get the disease.
She just passed it to her son.
© Milwaukee Journal Sentinal
By Lou Saldivar and Gary Porter
Sequencing Nicholas' DNA has given his family and doctors a diagnosis and more worries. Now they hope a new immune system can stop his disease.
By Mark Johnson and Kathleen Gallagher
For the first time in the three years of Nicholas Volker's illness, his mother dreams of the word she cannot say.In the dream, her 5-year-old, the little boy who calls himself "Batman," lies on the ground. There is a smile on his face. His blue eyes are closed. The heat is stifling and a boy and girl stand over Nicholas pointing down and holding their noses. Amylynne Santiago Volker keeps trying to wake her son, gripping his shoulders, crying his name over and over. "I can still hear myself screaming," she writes in her journal. "I hope and pray this is just my mind playing tricks on me."
The mother, a practicing Christian, believes in what she calls "signs and wonders." She pays attention to dreams, the sermons at church, the animals and scenery that catch her eye as she jogs. During her son's long stays at Children's Hospital of Wisconsin, she has prayed and fasted and slept beside him. She has not used "the 'D' word" and has bristled at the doctors who have.
So when the dream visits her in June of this year, on the eve of an important, but risky, treatment for Nicholas, it unsettles her to the core.
Nicholas has spent much of his life in the hospital, at times near death from a mysterious illness that attacks his gut. But a powerful new technology has allowed scientists to sequence his DNA, pinpoint the mutation causing his disease and arrive at an answer to the mystery.
A partial answer.
Sequencing revealed a more complex picture than the doctors at the Medical College of Wisconsin and Children's Hospital had suspected. The slightest mutation in a single gene has left Nicholas with not one, but two extremely rare, life-threatening illnesses.
One of them, called XLP, is an inherited immune system disorder that affects fewer than one in a million children. Found on the X chromosome, the disease strikes only boys and is usually fatal, rendering them unable to survive one of the most common human viruses, Epstein-Barr. Although Nicholas' specific mutation has never been seen before, it affects the same protein impaired in the other boys with XLP.
His second disease, the gut illness marked by holes that pierce the intestine and skin, has never been identified until now. Nicholas is the first known case in medical history.
A bone marrow transplant should treat XLP; doctors do not know whether it will remedy the gut disease.
The transplant will be a dangerous time for Nicholas. His old immune system must be wiped out using powerful chemotherapy drugs. His body could reject the cells that will build the new immune system. Even if his body accepts the cells, it will take time to create the new system and, in the interim, he will be vulnerable to any infection or virus.
The diseases could end his life; so could the treatment.
**
Nicholas Volker's name is unknown beyond his family, friends and medical staff, but his case has reached some of the world's elite geneticists. His sequencing, one of the first to result in a diagnosis, is hailed by some as a demonstration of what the Human Genome Project made possible a decade ago.
The Wisconsin scientists who decoded Nicholas' DNA are writing up the case for a medical journal. In late March, David Dimmock, a Children's Hospital genetics specialist, described the work at a meeting of the American College of Medical Genetics in Albuquerque, N.M. Dimmock explained the extensive search that took scientists from a list of more than 16,000 variations - departures from the normal genetic sequence - to the single one responsible for the boy's illness.
"It's thrilling to see that this has come around as a real consequence so soon because it took us the better part of 13 years to sequence the first human genome," said Francis Collins, director of the National Institutes of Health, who learned of Dimmock's presentation later.
"To now find, just a few years later, that it's possible to apply this in a medical situation and come up with an answer to a puzzling disorder of a child, is really remarkable and very gratifying."
Studies in late 2009 and early 2010 at Yale University, the University of Washington and other schools have shown success using the technique employed with Nicholas: sequencing not the whole genome, but a little more than 1% of it called the exons. Exons, part of every gene, contain the instructions for making proteins. Failure to make proteins correctly leads to many diseases.
These successes have come as scientists take stock of the genome project a decade after it gave us the first draft of our genetic blueprint. The accomplishment has spawned research into the genetic roots of diseases and commercial tests that reveal whether our individual mutations increase the risk of various ailments.
But the project has yet to bring about profound changes in medicine, such as cures for common illnesses or the sequencing-at-birth of babies
Scientists are learning that heart disease and other common illnesses appear to involve the interaction of several or even many genetic mutations, as well as diet, exercise and environmental factors. Sequencing offers simpler medical answers when it comes to rare inherited diseases such as those confronting Nicholas.
In his request to sequence the boy's DNA back in 2009, pediatrician Alan Mayer wrote, "a diagnosis soon could save his life and truly showcase personalized genomic medicine."
Doctors have reached a diagnosis and showcased genomic medicine.
Now, they must hope what they've learned can save Nicholas' life.
***
Allowing their son's DNA to be sequenced was an easy decision for Sean and Amylynne Volker.
The aftermath has been proving more difficult. Amylynne aches with the knowledge that she passed the ruinous mutation to Nicholas. Her extended family struggles, too. The mutation is a genetic shadow hanging over them all and over their children. It is like a sealed envelope no one wants to open.
To date, no other members of Amylynne's family have been tested for the mutation.
Even using the genetic information to treat Nicholas has not been as straightforward as the Volkers once imagined. They have not rushed to proceed with the bone marrow transplant.
After being hospitalized at Christmas, Nicholas recovered and came home. Late in March, the Make-A-Wish Foundation flew the family to Las Vegas, where Nicholas watched the monster truck world finals and met Batman. At school, he ran and climbed with the other children in gym class. In their Monona home, he roughhoused with Dad and bossed around his three big sisters.
To the Volkers, the days outside the hospital were a joy.
Still, all of Nicholas' food came through a tube. He longed for a bite of steak or pizza, but real food seemed to spur on the disease in his digestive system. The disease was the reason a short piece of intestine jutted from his stomach, diverting waste into a bag. Nicholas prayed for this nub of intestine to go back inside him, for his stomach to close up and for everything to be as it was before he got sick.
Conflicted as they were, the Volkers had signed the consent forms for the transplant.
By mid-June, the day was almost upon them.
"This is the best he's been," Sean said, admitting to second thoughts. "It's just so hard when he's so healthy and you're going to make him sick again."
***
On the morning after Amylynne's dream, the Volkers drive to Damascus Road Church, which sits in a small strip mall in Madison. It is Father's Day and Sean Volker carries his only son, slumped over his shoulder, into the church. The boy has spent each of the last three Father's Days in the hospital. The Volkers would like to spend this one anywhere else.
But Nicholas' face is ashen. His eyes keep closing. Dressed as usual in his Batman cape, the child appears bound for Children's Hospital once more - a day too soon. The next morning, Nicholas is due at the hospital to begin preparations for the transplant.
As the service opens, Amylynne stands, hands outstretched, eyes closed. Sean sits, Nicholas' head buried in his chest.
Family friend Dan Peck asks the congregation of 100 to pray for the Volkers. The family comes forward and Amylynne describes what Nicholas is facing.
"Pray against complications," she asks. "Pray that the new immune system will take, because Nic . . . "
Her voice falters. Friends surround the family, stretching their hands over Nicholas' head as he rests in his father's arms. A red spotlight bathes the child and the arms reaching toward him.
"We have your favor and we know that, God," prays Joseph Steinke, co-founder of this church in the Protestant evangelical tradition. "But we live in this broken and disrupted, unhealthy world. . . . Jesus, we're asking you to come and to place your hand on little Nic, and would you just guide him through this next week."
When the prayer finishes, the Volkers depart. Within an hour, Nicholas' fever passes. For once, the family avoids spending Father's Day at the hospital. They enjoy an afternoon of mini-golf.
That night Nicholas cannot sleep.
Put your arm around me, he tells his mom.
***
The next morning, the day he is scheduled for surgery to install a central line for chemotherapy drugs, Amylynne takes Nicholas straight to the emergency room. All the color has drained from his face. The fever is back.
"Water, Mommy," he pleads. "Get some. Get some. Get some."
But if the surgery is to proceed, he cannot drink. What happens next is up to David Margolis, the transplant doctor.
Margolis is a great believer in the fundamental principle: do no harm. He is also a stickler for proof, a trait instilled in him by his father, a lawyer. Before Margolis would agree to perform the transplant, a procedure that carries the risk of harm, he insisted his colleagues prove they had found the cause of Nicholas' disease.
He examines Nicholas and decides to postpone the surgery. The boy's symptoms suggest sepsis, the blood infection that almost killed him in the fall of 2007.
By nightfall, Nicholas is resting in intensive care, his mother hovering at his bedside.
Many times she has seen him gravely ill. Always, he has rallied. In the morning, Nicholas sits up and kisses her.
Mommy, I had a bad dream last night, he says. A scary ghost came into my room to get me, but then there was a younger man and he was in my room too and he said he would protect me in place of you.
In a few days, the sepsis clears. Margolis sets a new schedule. On July 14, Nicholas is to receive a transplant of umbilical cord blood from an anonymous donor.
Cord blood functions in a very similar way to bone marrow and is often given as an alternative in transplants. In Nicholas' case, Margolis prefers the cord blood because it carries less risk of graft-versus-host disease, a condition in which the transplanted cells turn against the recipient's body.
Even so, Margolis says, "There's a whole laundry list of things that can go wrong."
***
On the day before the transplant, mother and son discuss what's coming. Some who receive bone marrow transplants think of the event as a second birthday, the day their blood is reborn.
Amylynne explains the idea to Nicholas, who offers his own view. Until now he has been Batman. He has worn the bat cape and mask on many trips to the operating room.
Recently, though, he saw a sneak preview of the movie "The Last Airbender" and liked the character Aang, a boy with a shaved head who battles powerful forces.
Nicholas says he will go into the transplant as Batman. He will emerge as Aang.
After a week of heavy chemotherapy, he is ready. Though the chemo made him vomit, he seldom let it bother him. "Mom, I just got sick and I took care of it myself," he told Amylynne once when she returned to the room. "I got a bucket myself."
On the afternoon of July 14, a storm is simmering in Nicholas' room when the cord blood arrives in its plastic bag. One of the nurses has made a special Batman poster for the transplant, but the gesture fails to soothe Nicholas.
"Go away!" he screams even before the procedure begins. "I don't like the Batman sign. Take it apart."
Amylynne reminds him of his transformation from Batman to Aang. But he howls and will not be consoled. Though his father is working and cannot come until later, two of his sisters are in the room.
At 2:17, the nurse begins introducing the cord blood, a rose-red liquid that seeps from a 50-milliliter syringe through a line and into a vein in Nicholas' chest.
"We're starting, Bud."
Amylynne lies in the hospital bed beside her tense son as she has so many times. She is aware of an odd smell from the cord blood; it reminds her of creamed corn.
Nicholas' screams subside, fade to a whimper. He pulls her arm across his chest.
His face calms; his breath becomes slow and rhythmic.
She stays beside him, watching him drift off to sleep. Violins play. The soundtrack Amylynne has chosen begins with Vivaldi's "Spring" from "The Four Seasons."
At 28 minutes, Amylynne begins to weep. "I pray," she says, "that sickness and infirmity will have no place in his life." She reads from Psalm 107, beginning at verse 20: "He sent forth his word and healed them."
At 35 minutes, Vivaldi is replaced by "Aang's Theme," from the "Airbender" movie.
At 48 minutes, the last of the cord blood enters Nicholas. It is 3:05 p.m.
Minutes later, he sits up.
How do you feel? Amylynne asks. Any different?
Nope, he says
***
Eight days after the transplant, Nicholas' old white blood cells have vanished. The new donor cells are still traveling into the hollows of his bones, where they will begin making new red and white blood cells and platelets. His immune system is virtually defenseless. Sores form on his mouth, throat, tongue, gut. He has mucositis, a common reaction to chemotherapy.
Nicholas, his hair now shaved, barks at his mom. Stop talking. Don't ask any more questions.
Torrential rains whip through Milwaukee County that night and Nicholas' fever rises. His heart rate and blood pressure climb.
"Something is brewing in his body," Amylynne writes after meeting with Margolis.
There is talk of sepsis and fungal infections. Two weeks after the transplant, Nicholas' enemy has a name: adenovirus.
The virus strikes the respiratory tract. In a healthy person the symptoms might seem like a cold. In someone with a weakened immune system, the virus can be dangerous.
Nicholas insists he is not sick and demands toys, which Amylynne is no mood to deny him.
"What do you say to a kid who has lived over 600 days in the hospital," she writes, "has lived without food more of his life than with it, who has had over 150 trips to the (operating room), who has just had a transplant and can't go out of his room - now not even at night when everyone else is sleeping, even with a mask on?"
She copes by searching the Internet for information about each new complication. When she needs relief, she goes for a run.
By Day 20 after the transplant, the adenovirus is advancing. But there is good news, too: Nicholas' count of white blood cells has risen. The cells from the transplant appear to be engrafting
By Day 24, the adenovirus is declining. The white blood cell count grows. A pudgy smile lights up Nicholas' shaved head.
Then, on Day 29, after a week of encouraging news, Amylynne posts another urgent prayer request. Nicholas has a fever. He is struggling to remember things, even his mother's name.
He tests positive for HHV-6, a common virus that is a member of the herpes family. The virus can cause encephalitis, an inflammation of the brain, which is what worries Amylynne. His memory worsens. No sooner does he hang up the phone than he forgets which of his sisters was on the line
By Day 31, a test confirms that Nicholas has encephalitis. He lies in bed, his face blank. HHV-6 , encephalitis, memory loss - none is a normal complication from a cord blood transplant.
"There is no fight anymore with his cares, he just lays there, all docile and good," Amylynne writes. "I absolutely hate it and it breaks my heart."
Nicholas gets a rash. He gets graft-versus-host disease. He gets a staph infection.
The medical team anticipates problems and responds quickly - with antivirals for the adenovirus, HHV-6 and encephalitis; antibiotics for the staph infection; and an increase in immune-suppressing drugs for graft-versus-host.
In the cascade of bad news, it is the possibility of brain damage from encephalitis that worries Amylynne most. She longs to see the Nicholas who growled when he felt annoyed with a doctor or nurse.
Unable to sleep much, Amylynne feels tired and worried all the time.
"Losing his personality," she says, "if I knew this was coming, I probably wouldn't have done (the transplant). That's how I feel today."
A few days later, the personality begins to come back. Nicholas snaps at the anesthesiologist for touching his stuffed bull.
On Day 47, Aug. 30, Nicholas' memory is improving. He is healthy enough to eat real food for the first time in months, chicken noodle soup. He says it is the happiest day of his life. Two weeks later he is pouring sauce on top of a steak.
"The heavens are opening up," Amylynne writes on his Facebook page, "the angels are singing and Almighty God is dropping down bottles of A.1."
***
As Nicholas' body adapts to his new immune system, the Medical College installs a much faster, next-generation sequencing machine and awaits delivery of another.
The machine used to unravel Nicholas' DNA just a year ago is destined for a research lab.
Steve Turner, who founded Pacific Biosciences, a California company that makes one of the new machines, says the steps taken with Nicholas went against the prevailing view in medicine on the value of sequencing. "The thing I find stunning was the courage on the part of the physicians and the family to do this."
Nicholas' case, in his view, represents the beginning of an era in which our genes will be mined increasingly to find medical answers.
The change is likely to come with its own pitfalls and limitations. In many cases, genes may be only part of the picture along with factors such as diet, exercise and environment. Even when a disease is entirely genetic and when sequencing pinpoints the gene or genes responsible, doctors may have no treatment.
"One of the problems is: Without a therapy, do you want a diagnosis?" asks Walter Gilbert, an emeritus professor at Harvard who shared the 1980 Nobel Prize in chemistry for developing a method of sequencing DNA.
"It's a cost issue. Will somebody pay for it? For insurance to pay, it's not enough that the patient wants it or the doctor wants it, but the insurance company has to agree that it's useful in some way."
Some worry the flood of data from genome sequencing will overwhelm the storage capacity of our computers. Others are more troubled by privacy questions. Who will have access to the trove of genetic secrets, and how will access be restricted?
Still, Gilbert marvels that in half a century scientists have moved from a point at which genes "were still mysterious things . . . to the plethora of knowledge we have in modern biology."
More than a year has passed since Howard Jacob, head of the Medical College's Human and Molecular Genetics Center, received the e-mail asking to sequence Nicholas. He knows the next time doctors search a patient's DNA they may not connect a disease so definitively to one error or even several in the genetic code.
"We are a long way from saying this is something that is going to work every time," he says.
Yet he is confident this is where medicine is headed.
People ask how doctors will decide which patients to sequence. Jacob believes this will be a concern for only a year or two. A few years from now, he says, when the total cost hits $1,000 or less, the steps taken to diagnose Nicholas Volker's disease won't seem extraordinary at all.
The Medical College's new machines should have enough capacity, in theory at least, to sequence 90 entire genomes in a single year. Strange as it sounds, Jacob has told the dean that's not going to be enough.
"That's how fast this is changing," he says.
A sense of urgency about this new era of medicine crystalized for Jacob in the fall of 2009 during one of the meetings about Nicholas Volker. He thought of the young boy, and the second chance he might have because of what they were finding in his DNA.
Then he sprang from his chair and scribbled three words on the whiteboard in his office. He has left them there ever since.
"How many Nics?"
***
The Medical College has expanded its sequencing efforts. Six more patients are in various stages of the process.
"We learned a tremendous amount . . . that continues to ripple through our institution," the doctors wrote in a commentary accompanying their recent paper in the journal Genetics in Medicine.
Nicholas Volker was discharged from Children's Hospital on Oct. 21. Amylynne packed her van with plastic tubs stuffed with toys, games and Batman gear accumulated over the course of a four-month hospital stay.
Minutes before they drove away, a stranger in a shirt and tie rushed up accompanied by Margolis, the transplant doctor. Howard Jacob wanted to meet the boy whose genes he had come to know. Nicholas, less than a week from his sixth birthday, greeted the genetics expert, then poked him in the stomach with his plastic "Airbender" staff.
No one can be sure that sequencing Nicholas' DNA has saved his life. The cord blood transplant he received as a result should treat XLP, the rare immune system disorder.
But it is not clear what the transplant will mean for the mysterious illness that ravaged his intestine and it may be two years before doctors know, says pediatrician Alan Mayer. After all, the gut disease did not show itself until two years after the boy was born.
Today, Nicholas is a new patient. Inside his body are two distinct DNAs, one with the mutation and one without it.
His immune system has the donor's DNA - no mutation. The rest of his body has the DNA he was born with, including the slight genetic error that caused so much damage.
Mayer wonders how all of this will play out - Nicholas' new immune system co-existing with his old gut.
The doctor likes to imagine a time when the boy is healthy enough to watch a Brewers baseball game. When the years in the hospital, the surgeries, the feeding tubes are all a vague memory.
He sees a summer day, and Nicholas Volker at the ballpark eating a hot dog.
© Milwaukee Journal Sentinal
By Alison Sherwood
By Alison Sherwood
By Alison Sherwood
Biography

Mark Johnson is a reporter at the Milwaukee Journal Sentinel. He twice been part of reporting teams that were finalists for the Pulitzer Prize in explanatory reporting, in 2003 and 2006. He won two Inland Press Association awards, a Missouri Lifestyle Journalism Award and the 2009 Communications Award from the National Academy of Sciences. He was a finalist for the 2010 American Society of News Editors Award for nondeadline writing. He also has been a finalist for a Taylor Family Award for Fairness administered by the Nieman foundation and has received the top award for feature writing from the American Association of Sunday and Feature Editors. Johnson joined the Journal Sentinel in 2000. Previously he worked for the Provincetown (Mass.) Advocate, The Haverhill (Mass.) Gazette, the Rockford (Ill.) Register Star and The Providence (R.I.) Journal. At the Journal Sentinel, he has traveled to Florida to cover the 2000 presidential ballot controversy, to New York to cover the Sept. 11 attacks and to Houston to cover the space shuttle Columbia disaster. He now covers health and science.

Gary Porter has been a photojournalist with the Milwaukee Journal Sentinel since 1984. He has worked on many award-winning stories, including the ground breaklng "Made in China" series that helped explain the relationship between what is happening economically and socially in China and the loss of jobs and business in Wisconsin. Porter also won an Oversees Press Club award in photojournalism and a United Nations World Hunger Year Award, as well as a National Press Photographers Association award for his photographs from "Empty Cradles: The Global Tragedy of Child Mortality," for which he photographed in India, Nepal and Bangladesh. Porter has also been chosen as the Wisconsin News Photographer of the Year five times while he has been at the Journal Sentinel. Other recent major stories include the last Hmong migration from Thailand to the United States, chronic wasting disease and foot-and-mouth disease in the U.K. Porter attended the University of Wisconsin system and studied photography at Ryerson University in Toronto.

Kathleen Gallagher is a business reporter at the Milwaukee Journal Sentinel. She won a first-place award for explanatory reporting in the 2006 Inland Press Association contest. Gallagher has a graduate degree in English from the University of Illinois at Chicago. She was a communications consultant at the Federal Reserve Bank of Chicago and a writing instructor at the American Institute of Banking in Chicago before joining the Milwaukee Sentinel in 1993. At the Journal Sentinel, Gallagher has investigated the operator of a multistate cattle Ponzi scheme, traveled by helicopter with professional investors to visit oil rigs in the Gulf of Mexico and looked into microscopes at a Madison, Wis., company that sells stem cell-derived heart cells to pharmaceutical companies. Gallagher now covers investments and Wisconsin's life sciences and other emerging, high-growth industries.

Lou Saldivar is a visual journalist and graphics editor for the Milwaukee Journal Sentinel. He has won awards from the Society for News Design and the Milwaukee Press Club. He contributed graphics to stories that were recognized with Pulitzer Prizes in 2008 and 2010. Saldivar holds a master's of fine arts degree from the University of Wisconsin-Whitewater.

Alison Sherwood is a multimedia producer and blogger for the Milwaukee Journal Sentinel. She has received a Milwaukee Press Club award for multimedia storytelling as well as awards from the American Association of Sunday and Features Editors and the Association of Food Journalists for her blog, Post-College Kitchen. She holds a bachelor's degree in journalism from the University of Missouri and is a member of Kappa Tau Alpha National Honor Society, Omicron Delta Kappa national leadership honor society and Zeta Tau Alpha fraternity.